
A new report says the system is failing and that the digital tools meant to help are part of the problem. But technology, done properly, could also be part of the answer.
The Gap Nobody Likes To Talk About
There are 826,000 people living with dementia in England and only 38 per cent of social care staff have completed condition-specific training.
By 2040 that figure is expected to reach 1.2 million, with around 70 per cent of care home residents already living with diagnosed or undiagnosed dementia.
Yet the workforce responsible for caring for those people is still not receiving adequate training to do that job well.
A new report The Training Gap: A Hidden Injustice In Dementia Care And How To Fix It, produced by Leeds Beckett University and commissioned by Alzheimer’s Society makes that case with evidence that is difficult to argue with.
Drawing on a national audit of 53 providers covering 119 training packages and a direct survey of 184 care workers, it describes a sector where good intentions have consistently failed to produce adequate outcomes.
Oonagh Smyth CBE, Chief Executive of Skills for Care, writes in the report’s that, “the training being delivered isn’t always dementia specific or at the right level,” adding that it is “often not delivered in ways that we know to be more effective for promoting learning.” Coming from the organisation that leads workforce development strategy for the entire sector, that is a significant admission.
What The Numbers Show
The national benchmark is the Dementia Training Standards Framework, which sets out three tiers. Tier 1 is basic dementia awareness, the minimum for any health or care worker. Tier 2 covers the knowledge and skills required by staff in regular direct contact with people living with dementia, across 11 additional topics including person-centred care, communication and behaviour, and end of life care. For hands-on care staff, Tier 2 is the standard. Most are not reaching it.
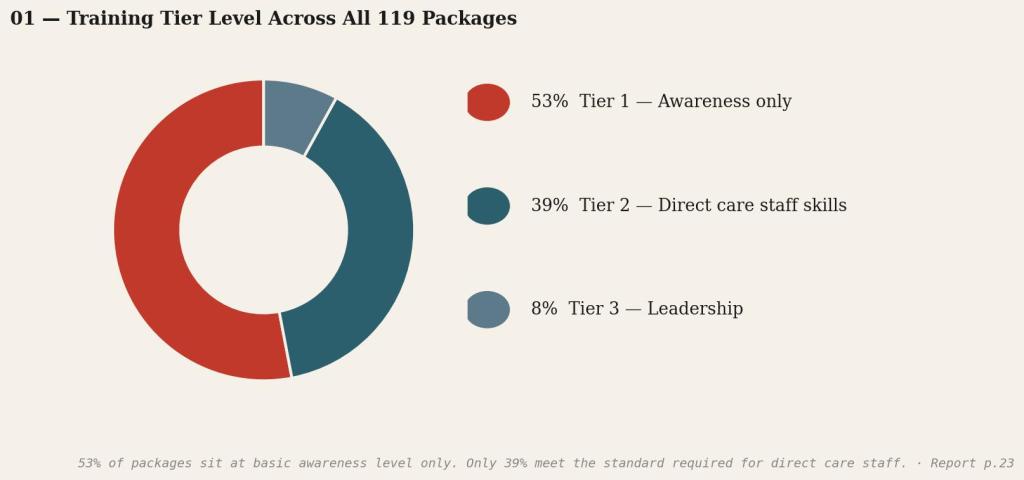
The report found that 53 per cent of training packages sit at Tier 1 awareness level only. Just 39 per cent of available training was designed to deliver the knowledge and skills required for direct care staff.
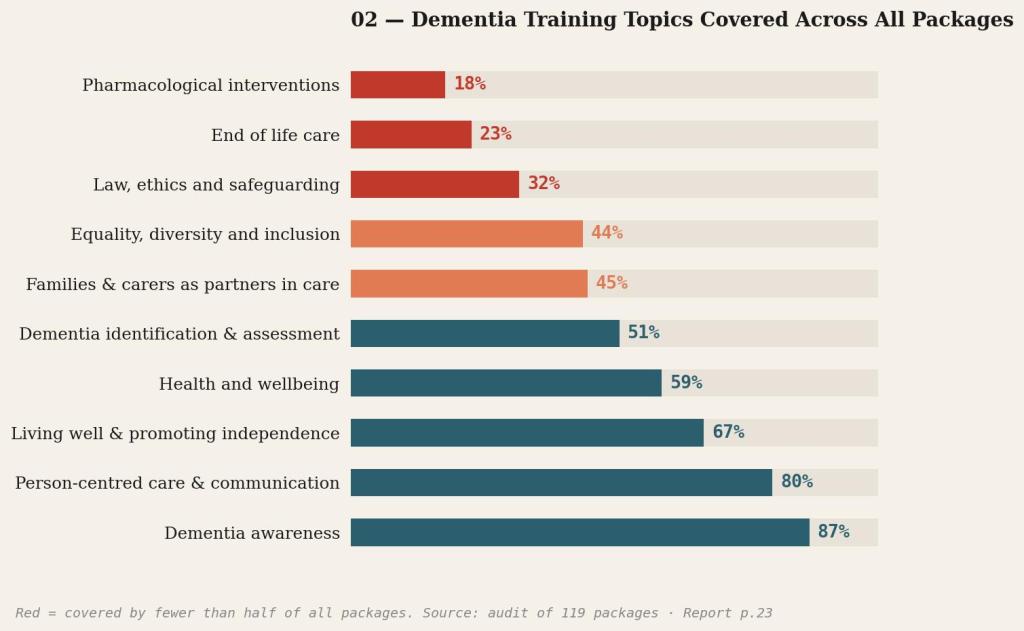
The most critical topics are the ones most likely to be absent, end of life care appears in only 23 per cent of packages working with families and carers as partners in just 45 per cent. Only 47 per cent of staff said dementia training was included in their induction meaning more than half begin working with dementia patients without any targeted preparation.
The report’s Lived Experience Involvement Group people living with dementia and unpaid carers who helped shape the research put it plainly, “You wouldn’t expect to have heart surgery from a surgeon who only had an awareness of how the heart works.” The comparison is blunt but it is also applicable.
Where Technology Has Made Things Worse
The specific role that digital training has played in creating this situation deserves attention, because it has functioned less as a training tool and more as a mechanism for generating evidence of compliance without delivering actual competency.
The report found that 51 per cent of training packages were completed using e-learning with no live interaction, and 43 per cent used e-learning as the only method of delivery. Seventy-one per cent of those e-learning packages were at awareness level only. On duration, 50 per cent of all packages offered just one to two hours of dementia-specific content. Only 15 per cent met the best practice threshold of eight hours or more and among e-learning packages specifically, 67 per cent lasted just one to two hours.
Assessment is equally lacking. Only 37 per cent of packages had been evaluated for their impact on staff. Where assessment did exist, 98 per cent took the form of quiz-style knowledge checks. Two per cent included anything as demanding as role play.
This has happened because e-learning is cheap and easy to record. In a sector under serious cost pressure, that combination is attractive. But the cost of inadequate training is eventually endured by people living with dementia and by staff asked to manage complex situations without adequate preparation.
The Legal Pressure Building
The report’s central recommendation is a new legal requirement, all direct care staff in older adults’ care, across care homes and home care, must complete best practice dementia training of at least eight hours mapped to Tier 2 of the Dementia Training Standards Framework enforced through CQC statutory guidance under Regulation 18.
For providers, that would make the current dominant model non-compliant. Short e-learning modules, awareness-only content and no facilitation would no longer be sufficient. The sector will need scalable, evidence-based training solutions and it will need them fast.
What Better Technology Actually Looks Like
The report’s critique is not of technology itself but of a particular, impoverished application of it. The best practice framework it calls for interactive, evidence-informed, facilitated, at least eight hours in total is entirely compatible with digital tools. It just demands very different ones from what most providers are currently using.
The most immediate gap is retention. A worker who completed a dementia module three months ago has, without reinforcement, likely retained very little of it. Spaced repetition platforms address this directly, delivering short, targeted knowledge prompts at calibrated intervals rather than treating training as a single event.
Adaptive learning systems go further, assessing what each individual already knows and adjusting content accordingly. The report found that 63 per cent of training is delivered uniformly to all staff regardless of role or experience. Platforms that personalise at scale offer a more effective alternative.
The empathy and communication gaps identified in the report are harder to address through conventional formats, which is where virtual reality has attracted serious interest. Providers including Embodied Labs have developed first-person immersive simulations placing care workers inside the subjective experience of dementia navigating environments that have become confusing, struggling to follow conversation, experiencing the disorientation that often underlies the behaviours staff find hardest to manage.
Early evidence from care settings suggests meaningful improvements in empathic understanding and communication practice, and the cost and accessibility barriers to VR are falling.
End of life care present in just 23 per cent of packages and one of the most consequential gaps in the current picture is a topic the sector has struggled to teach at scale because it requires both emotional preparation and the ability to practise difficult conversations.
AI-driven conversational simulation, where staff rehearse sensitive exchanges with a responsive simulated patient or family member and receive structured feedback, offers a credible and scalable response. It cannot replicate a skilled human facilitator, but as a tool for building confidence before staff encounter these situations in practice, it fills a gap that currently goes largely unaddressed.
Home care staff explicitly included within the proposed legal requirement present a particular challenge. They are dispersed, shift-based and without regular access to a fixed workplace. Mobile-first microlearning platforms built for smartphones, accessible offline, designed to fit around shift patterns rather than requiring desk time, are specifically suited to this population. Used as part of a broader blended strategy, they address a structural problem conventional training has never resolved.
Technology Is Not A Shortcut
None of this works in an organisation that does not take training seriously. The report identifies strong leadership as one of its five core components of best practice training, and the data bears out that most providers are not building the internal culture and expertise that makes any training investment stick.
The sector has been reaching for digital tools as a way of managing a training obligation at minimum cost. That approach has produced the current situation, a workforce that has technically completed training, knows what a quiz answer should look like, and is still not adequately prepared for the job. Better technology deployed in the same spirit will produce the same result.
What needs to change is the underlying expectation. Platforms are only as good as the organisational context they operate in. A provider that protects learning time, follows up on what staff have covered and treats training as genuine professional development will see very different outcomes from the same tools as one that does not. Given that a legal mandate may be on its way, that distinction is about to matter considerably more than it does today.
