
As pre-hospital ECMO trials gather momentum internationally, the implications for community health services and urgent care delivery are profound, raising urgent questions for NHS commissioners and care technology innovators about what truly advanced care in the home could look like.
When The Hospital Comes To You
For decades, the boundary between hospital-grade intervention and community care has been defined largely by geography and infrastructure. Intensive care units required fixed equipment, specialist teams, and controlled environments. That assumption is now being dismantled not gradually, but dramatically by a new generation of portable clinical technology being trialled in pre-hospital settings.
The latest and perhaps most striking example comes from Melbourne, Australia, where Ambulance Victoria and The Alfred hospital have successfully deployed extra-corporeal membrane oxygenation ECMO inside a patient’s home. Peter, a 56-year-old father, suffered a cardiac arrest in March this year. After more than 20 minutes of CPR and nine defibrillator shocks, a specialist team performed emergency surgery on his living room floor, connecting him to a portable ECMO machine that replaced the function of his heart and lungs while he was transported to hospital. He survived.
What ECMO Is And Why It Matters
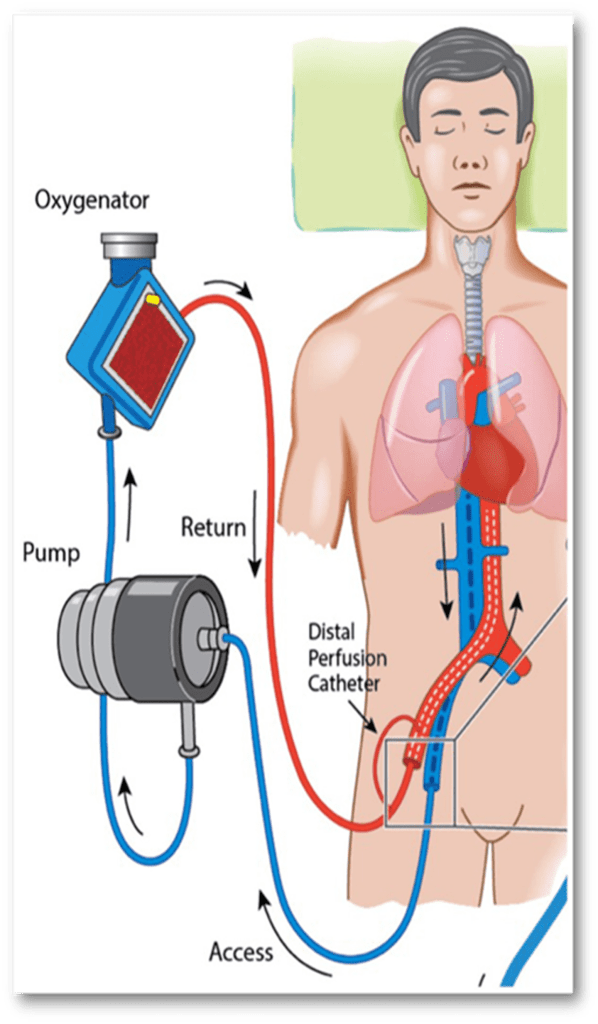
ECMO is a life-support intervention that circulates blood outside the body, oxygenating it and returning it to the patient. Until recently, its complexity placed it firmly in the domain of hospital intensive care units. The machinery is intricate, the procedures invasive, and the clinical expertise required considerable. Deploying it in a domestic setting was, until very recently, inconceivable.
Melbourne is now the first city in Australia and one of a small number globally to operate a pre-hospital ECMO programme. Peter was the 41st patient to receive the treatment outside of hospital under the CHEER3 trial (CPR/pre-Hospital/ECMO/Emergency Reperfusion trial 3), a research programme funded by The Alfred Foundation and Ambulance Victoria.
The survival implications are significant. Research published in connection with the trial indicates that cardiac arrest patients who do not respond to standard resuscitation face a survival rate of roughly four per cent. Pre-hospital ECMO, according to international evidence cited by the programme, may push that figure towards 30 per cent.
As Ambulance Victoria’s Executive Medical Director, Associate Professor David Anderson, stated in the programme’s release: “Highly skilled ECMO teams are bringing cutting-edge technology from the hospital intensive care unit directly to patients in life-or-death situations, delivering critical care faster and potentially giving more patients a better chance of survival and recovery.”
Pressure On Community Services And The Case For Innovation
NHS England has made the shift towards care closer to home a central plank of its long-term strategy, with integrated care systems tasked with reducing avoidable hospital admissions and delivering more urgent care in community settings. Yet the clinical technology available to paramedics and community teams has struggled to keep pace with that policy ambition.
British paramedics already carry advanced airway management tools, point-of-care diagnostics, and increasingly sophisticated monitoring equipment. But the gap between what is clinically possible in a hospital and what is achievable on a doorstep remains vast. Pre-hospital ECMO, as demonstrated in Melbourne, suggests that the gap is not fixed; it is an engineering and organisational challenge, not an absolute clinical boundary.
For NHS ambulance trusts, integrated care boards, and the social care technology companies increasingly embedded in community health pathways, this should be cause for serious attention. The UK’s ambulance services have invested in specialist critical care paramedic roles and physician response units in recent years, establishing the clinical workforce infrastructure that would, in principle, be needed to support programmes of this kind.
Home Care Technology And The Expanding Definition Of Clinical Space
Care in the home is no longer simply about maintaining stable conditions or providing companionship and personal support. An emerging ecosystem of clinical-grade, portable, and increasingly connected devices is making it possible to deliver interventions that would once have been unthinkable outside a hospital. From wearable cardiac monitors that feed data to NHS virtual wards, to portable ultrasound devices used by community practitioners, the trajectory is clear: the home is becoming a clinical environment.
ECMO is, admittedly, at the extreme end of that spectrum. It requires a team of intensive care physicians and specialist paramedics, not a lone district nurse. But its pre-hospital deployment is a bellwether for the direction of travel.
A Future Where The ICU Follows The Patient
The image of a specialist team setting up a heart-lung bypass machine on a family’s lounge floor is arresting precisely because it disrupts every assumption we hold about where serious medicine happens. It is also, in many respects, the logical endpoint of a direction the UK care sector has already committed to: bringing care home.
What the Melbourne trial demonstrates is that with the right workforce, the right technology, and the right research infrastructure, the boundaries of what is achievable in community and home settings can be pushed far further than current practice suggests. Pre-hospital ECMO may remain a niche intervention for some years. But the principle it embodies that critical, life-saving care technology can travel to the patient rather than the patient travelling to it is one that will increasingly define the future of community health technology in the UK and beyond.
For care providers, NHS leaders, and the innovators building the next generation of home care technology, Peter’s story is more than a remarkable human interest piece. It is a glimpse of what becomes possible when clinical ambition, technological capability, and coordinated emergency response align and a marker of how far the UK care sector still has to travel to reach that frontier.

